Caption: Yes. To lower LDL cholesterol, medications of oral tablets as well as injectables are available. Regardless of the excitement on the availability of the highly efficacious PCSK9 inhibitors, statin therapy are still the undisputable top choice.
A Vigilant note: A recent seemingly scholarly presentation on the topic of Cholesterol: A friend or foe, has been circulating around through WeChat Channel. This presentation advocates high cholesterol diets and savages the benefits of statin therapy. His claim is basically a replay a old drama from almost 10 years prior, which were sent to academic graveyard due to overwhelming research evidences. This presentation is deceiving and harmful. Works may be necessary to address how a deceiving presentation looks so convincing.
Statin associated muscle symptoms (SAMs) occur in 5 – 15% of patients treated with a statin. Nine percent abandon statin therapy because of muscle symptoms. Generally, this is described as statin intolerance. Statin intolerance can be differentiated into statin true intolerance and statin pseudo-intolerance (or partial intolerance). Ninety percent of patients of statin intolerance are statin pseudo-intolerant. They experience muscle symptoms when starting a statin, but are able to continue statin therapy as symptoms subside. All statin associated symptoms are reversible.
If you experienced muscle pain after starting statin therapy, you may have several options:
- Abandon your statin treatment- consequently your risk of atherosclerotic cardiovascular events increase.
- Replace your statin with a non-statin drug tor LDL- Non-statin LDL lowering drugs of oral route have lower efficacy than statins in LDL reduction.
- Attempt to continue your statin treatment by:
- Identify and eliminate risk factors of SAMs- For example, avoid strenuous physical activities like weight lifting, marathon races.
- Take the vitamin supplement CoQ10. Consider Vitamin D.
- Switch to a different statin drug. Rosuvastatin and pravastatin have been reported have much less muscle symptoms than other statins. Simvastatin is the worst (Ref. Natalie ward).
- Start statin re-challenge strategy- this approach includes dosing adjustment or switch to another statin.
The collective measures to help the continuation of statin therapy is termed “Take your time approach” and “Step by step approach”. This approach is strongly advocated by all experts and guidelines.
People with existing risk factors predispose a patient to statin associated muscle symptoms
Intrinsic risk factors include age older than 70, female sex, Asian ethnicity, existing kidney or liver disease, or low body mass. They are inherently difficult to modify. It is known that all major side effects of statins are dose- dependent, meaning that higher dose produces more severe side effects. For the patients bearing those risk factors, a lower dose may be considered at the initiation of statin therapy. One practical strategy is incremental dosage titration, gradually to reach the maximal tolerated dosage (Ref. Steve Nissen, podcast).
Other risk factors are extrinsic and modifiable. Identifying and eliminating those extrinsic modifiable risk factors is first step in the prevention and treatment of statin intolerance:
- High-dose statins- High dose statin regimens reduce risk of cardiovascular events the most, but also cause higher rate of intolerance. These regimens include 40-80mg atorvastatin, 40-80mg simvastatin. “Low to moderate” dosages may be defined as less than half of labeled maximum dosage, such as less than 40mg atorvastatin. The muscle side effects of statins at low to moderate dosages are similar to those of placebo, meaning “almost no side effects”.
- Drug interactions– Except pravastatin and rosuvastatin, other statins are metabolized by a liver enzyme called CYP 450. Certain medications inhibit this enzyme, which lead to unusually high amount of a statin in our body system. As a result, a patient concurrently taking these medications with a statin may be more prone to muscle symptoms. For example verapamil, a common medication for cardio arrhythmia, increases simvastatin in our body system by 4-6 fold. A common antibiotic, erythromycin also increases simvastatin by 4-6 fold. Cyclosporine, an immunosuppressant for organ transplant, increases simvastatin by 10-20 fold. The list of medications interacting with statins is long. Using pravastatin and rosuvastatin may be better options with risks of major drug and drug interactions.
- Hypothyroidism– Patients with untreated hypothyroidism have higher rate of statin intolerance. According to lipid management guidelines, hypothyroidism must be ruled out before treatment with lipid-lowering medications like statins. Hypothyroid patients are required to re-evaluate their lipid profile when their thyroid hormone level reaches the normal range. Patients with hypothyroidism usually have high levels of total and LDL cholesterol, because low thyroid hormones impair our normal cholesterol metabolism. Bringing thyroid hormones back to the normal range can lower the levels of total and LDL cholesterols.
- Grapefruit can inhibit the body’s clearance of simvastatin, atorvastatin or lovastatin, similar to the drug and drug interactions mention above. Thus, large intake of grapefruit juice increases statin side effects.
- Vitamin D deficiency Replenishing vitamin D for a patient may improve statin associated muscle symptoms. The role of Vitamin D in treating muscle symptoms is intricate. Cholesterols is the precursor in Vitamin D synthesis. One of the early signs of osteoporosis due to Vitamin D deficiency is body ache.
- Alcohol abuse, excessive physical exercise They are the risk factors worsening muscle symptoms of statins.
Most of the risk factors increase side effects of a statin because they drastically increase of the amount of statin in our body. After identifying risk factors, muscle side effects may be reconciled by dosage adjustment. For example, if a patient is taking diltiazem, a popular calcium channel blocker, for her atrial fibrillation, it is recommended a dosage adjusted to 10 -20 mg atorvastatin, which is less than ¼ of its maximum dosage (Ref. Clark Gillett). Slimmer Asian ladies have the risk factor of low body mass, and may start at a lower dosage than regular recommended dosage, followed by upward titration to max tolerated dose.
In choosing a medication to lower LDL cholesterol, the prominent expert, Dr Steve Nissen has told his physician audience to follow “step 1 –a statin, step 1—a statin, step 3 – still a statin”. Meaning that when muscle symptoms occur, you can change dosage, or another medication, but your choices are still a statin. You should not abandon statin therapy quickly.
There are several strategies of continuing statin therapy when statin associated muscle symptoms occur.
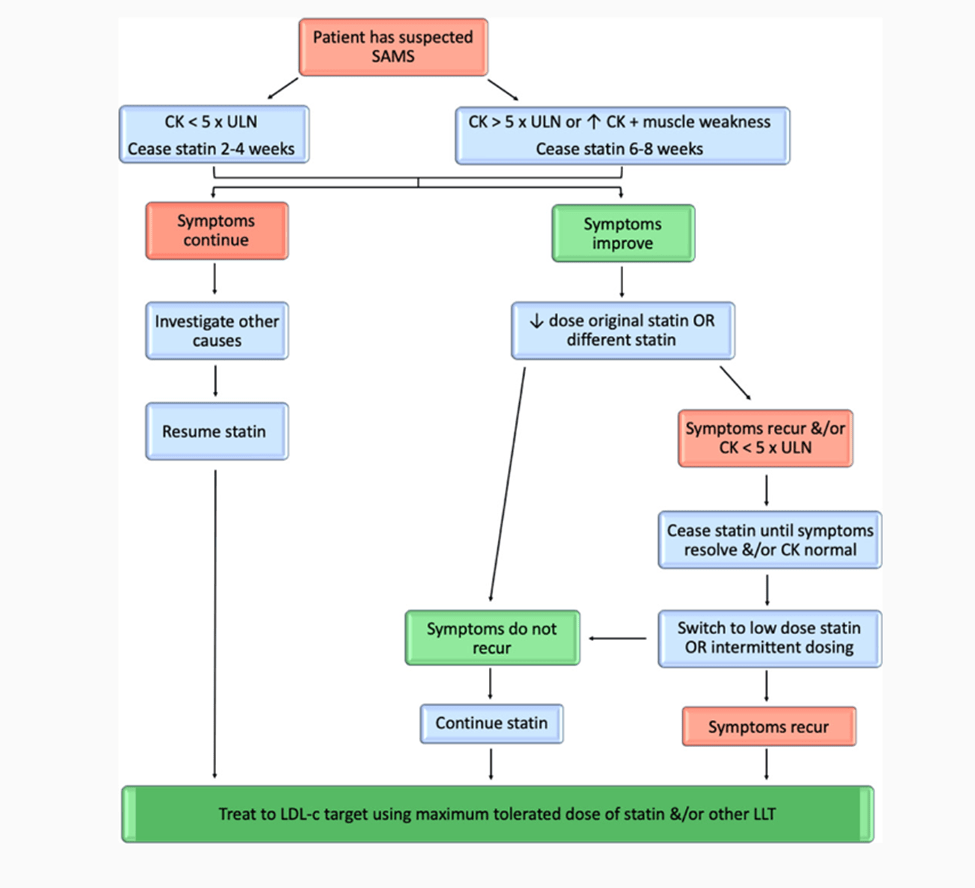
Statin Re-challenge This strategy of statin re-challenge is most recommended. It can differentiate a patient from true statin intolerance. Thus, a patient of pseudo statin-intolerance can confidently continue her statin treatment. After discontinuation of statin for 6-8 weeks, muscle symptoms usually resolve. Then the patient restarts the same statin at lower dosage, or start a different statin. Patients and clinicians should be aware that even if patients experience muscle symptoms with 1 statin, they may not experience those with another statin. From all studies, it is the overall consent that high percentages of patients were able to resume statin therapy using the strategy of re-challenge. For a patient with mild to severe muscle symptoms, various algorithms of statin re-challenge are available for clinicians to refer (Link).
Intermittent Dosing In this strategy, a patient takes a statin every other day. The effectiveness of the strategy to lower LDL cholesterol is, however, 15% less than regular daily dosing.
Concomitant regimens of a statin with a non-statin LDL cholesterol lowering drug This strategy is applied when a patient needs to further lower her level of LDL cholesterol, but the patient is already in her maximally tolerated statin dosage. Ezetimibe added-on to simvastatin is able to further lower the LDL levels by 25%. Because the synergic effect of the combination, a low dosage of simvastatin with an added-on ezetimibe is able to have the efficacy of reducing the LDL Cholesterol close to that of moderate dosage of simvastatin used alone. Ezetimibe is the first line of non-statin in this strategy. Bile acid sequestrants (cholestyramine etc.) and PCSK9 inhibitors can be considered as added on to statin therapy. Alirocumab and evolocumab are the two available PCSK 9 inhibitors. They are injectable, highly efficacious LDL cholesterol lowering drugs. PCSK 9 inhibitors added to a statin are able to reduce LDL cholesterol another 50%, and significantly further reduce risk of cardiovascular events. Most recently new drug bempedoic acid is approved to use in conjunction with statin.
Vitamin Supplement of CoQ-10 In the process of lowering LDL cholesterol, statin also lower CoQ-10 level in our body system, resulting in its deficiency. 100 or 200 mg CoQ 10 daily supplement has been suggested to reduce the muscle symptoms.
Non-Statin LDL cholesterol lowering drugs For a patient of true statin intolerance ezetimibe is the first option. New drug Bempedoic acid is expensive and its efficacy is similar to ezetimibe. PCSK9 inhibitors are great for a patient of high CV risks, with the cost more than $400 per month. There are several other groups of non-statin LDL lowering drugs. Bile acid sequestrants include cholestyramine, coleserlam . Fibrates include fenofibrate, gemfibrozil. Niacin is available indifferent dosage forms. Those drugs used to be the drugs of choice once upon a time before statins was developed. Now their roles in LDL lowering therapy are in declining due to their low efficacy in the reduction of LDL, low or no benefits of reducing CV risk or serious side effects. Therefore, they are not in my interest in this writing. However, I can’t help to mention a scientifically breakthrough new medicine, called inclisiran. It is the first medicine made of RNA (small interfering RNA or siRNA) in the history of the drug development. Another piece of miscellaneous information is about Over-the-counter supplement called Red Rice Yeast. Many people are afraid of side effect from prescription statins, so they turn to herbal medicines. However, they do not know that the active ingredient of Red Rice Yeast is still a statin, lovastatin.
Understanding CV benefits of statin compared to ezetimibe may help continuation of statin therapy
In responding to the complain of statin associated muscle symptom, the common short cut of bypassing the recommended “ Step by Step” approach is to replace statin with a non-statin LDL lowering drug. Ezetimibe is usually the pick. Replacing a statin with ezetimibe renders a patient the sense of complacency. FDA has not recommended use of ezetimibe in primary prevention and as monotherapy because of lack of outcome data. Perhaps, an independent minded friend may take a stance like “as long as ezetimibe lowers my cholesterol, and I am not troubled with muscle pain, I would cares less about what FDA said”. To convince this friend to continue statin therapy, statin and ezetimibe have to be compared shoulder to shoulder, with a strong contrast. Unfortunately the outcome of reducing CV risk for ezetimibe used alone is not available, neither for ezetimibe in primary prevention.
Ezetimibe used in combination with simvastatin:
-in comparison with a placebo used with simvastatin (equal to simvastatin used alone) for 7 years
A – The combination prevents one CV event for every 50 patients treated for 7 years (the result from simvastatin used with placebo is the base line).
B – 11% relative CV risk reduction.
C – No improvement in mortality (Ref. IMPROVE- IT Trial) .
A statin (rosuvastatin):
A –The 0.59 CV events were prevented statin vs placebo for every 100 patients per year of follow up. ( derived to 2 CV events prevented for every 50 patients treated for 7 years)**
B– The relative CV risk reduction almost 50% (Link).
C -12 % reduction in all-cause mortality after 5 year statin therapy per mmol/L (38mg/dL) reduction in LDL. (Ref. P. Toth)
** This extrapolated calculation needs validated as I assumed a linear relation.
One direct comparison is the efficacy of lowering LDL:
Ezetimibe used alone is able to lower LDL by 18%, statins can lower LDL by up to 50%.
It is the general consent that every 1 mmol/L(38.7mg/dL) of LDL reduction is associated with a 22% relative risk reduction in major cardiovascular events. According to this formulation, the benefits of statin in reducing the CV risk would be more than 2 folds better than that of ezetimibe in theory.
Final comment
When I have muscle symptoms after stating a statin, all efforts should be made to continue my statin therapy.
Key Reference:
Statin Toxicity, Natalie C. ward et al. Circulation Research,2019, 124:328
Lipid management guideline Connie Newman et al. JCEM October 13 2020
Persistent Dyslipidemia in Patients with Hypothyroidism: A Good Marker for Personalized Replacement Therapy? Bernadette Biondi The Journal of Clinical Endocrinology & Metabolism, Volume 104, Issue 2, February 2019, Pages 624–627, https://doi.org/10.1210/jc.2018-02302
Association Between Lowering LDL-C and Cardiovascular Risk Reduction Among Different Therapeutic Interventions–A Systematic Review and Meta-analysis, Michael G. Silverman et al. JAMA. 2016;316(12):1289-1297. doi:10.1001/jama.2016.13985
An Evidence-Based Guideline for Treating Dyslipidemia in Statin-Intolerant Patients Dylan Lempp; The Journal for Nurse Practitioners Vol 17, Issue 8, September 2021, Pages 910-915
Considerations for Safe Use of Statins: Liver Enzyme Abnormalities and Muscle Toxicity , R. CLARK GILLETT, et al. Am Fam Physician. 2011, 83(6):711
Can Fam Physician. 2015 Mar; 61(3): 25 Does ezetimibe modify clinical outcomes? Ricky D. Turgeon, ACPR et al. (Ref to Cannon CP-IMPROVE-IT Trial)
Management of Statin Intolerance in 2018: Still More Questions Than Answers Peter P. Toth, American Journal of Cardiovascular Drugs Published: 09 January 2018 volume 18, pages157–173 (2018)
Statin-associated muscle symptoms (SAMS) management algorithm
—Source: Statin Toxicity, Natalie Ward, Circulation Research, Vol 124, No 2 , 2019