Caption: ASCVD Risk Estimator Plus is a computer based tool, designed for assisting physicians and patients to assess the risk of atherosclerotic cardiovascular events. Based on the results of risk assessment, advices of medical treatment are provided to reduce the risks. >
Have you ever, like me, known someone in your life who was a victim of heart attack or stroke? It is heart-wrenching to learn a beloved family member, a friend of childhood or a college classmate struck by these brutal diseases. In the past when the understandings of these diseases were lacking, effective medicines were not available, people were basically powerless in confronting these disastrous attacks. At present, we have better knowledge, and we have very effective medicines. The scientists of National Institute of Neurological Disorders and Stroke have unequivocally informed us that 80% of risk factors causing stroke are controllable [Link]. 80 percent, what an astonishing number is! My understanding to this number is that, if we follow good, scientific advices (not the fake ones), our probability of having a stroke-attack would be reduced by 80%. This is the power of primary prevention. ASCVD Risk Estimator Plus is a tool of helping people to know if they need a primary prevention, and to obtain advice of drug therapy.
Thus, knowing the levels of our current plasma cholesterols is critically important. At present, fortunately, it is quite convenient to obtain such information. In addition to the orders of the lab tests placed by physicians, we are able to place an order online for ourselves without visiting physicians’ office. If you search the internet using the keywords “order my lab test”, you would see the availability of the test. The test is inexpensive, provided by chain clinical labs, which are located all over in every towns and cities in U.S. .
Without history of heart attack or stroke, who should start a preventive statin therapy?
If a person had been clearly diagnosed of hypertension, high cholesterol or diabetes, she would be usually smart enough to seek for medical treatment. However, there are situations that we may be unsure if a drug therapy is necessary. The difficulty of making treatment decision is due to various reasons. Examples are when blood pressure, blood glucose, or cholesterol is just marginally high in borderlines. Statins are drugs used to lower LDL cholesterol. When their LDL cholesterol levels are not high, many diabetic patients, or even physicians sometimes, do not realize that they still need statin medication to reduce the risk of heart attack or stroke. In anti-hypertensive therapy, the goal for lowering blood pressure has been the level of less than 130/80. Recently it is recommended less than 140/90 by Am Academy of Family Physicians guidelines. (Am Fam Physician. 2022 Dec;106 (6):On line). If my blood pressure happened to be 135/85, between the ranges of the two different goals, should I start anti-hypertensive drug treatment? There are many other circumstances of uncertainty affecting patients as well as clinicians in decision-makings.
The rational for a decision-making is based on the predicted improvement of outcome from a medical treatment. In statin therapy, the outcomes are measured with its effectiveness to prevent atherosclerotic vascular events (heart attack or stroke). The approaches of prevention are classified into primary prevention and secondary prevention. The secondary prevention is to start the medications for those who have had history of heart attack, stroke, or high cholesterol, in order to prevent the re-occurrence of those events. Primary prevention is to start the medications for those who have no history of heart attack, stroke or other atherosclerotic events, in order to prevent the future occurrence of those events.
Statins in secondary prevention undoubtedly improve the outcome for patents. However, the benefits of statins in primary prevention is required much subtler assessment. Giving another scenario, a person has borderline of LDL cholesterol, without history of cardiovascular events. He is a smoker, and hypertensive, should he start a statin as a primary prevention? Most of us would probably dismiss the idea of statin therapy. However, this may lead to missing the opportunity of preventing a future heart attack, according to clinical evidence.
That challenge of deciding primary prevention for anti-hypertensive therapy is similar to that of statin therapy.
What is ASCVD Risk Estimator Plus
ASCVD Risk Estimator Plus, a computerized-program has been designed for helping patients and physicians to decide whether medications are needed
ASCVD Risk Estimator Plus is a computer based tool. It has been developed by the most prestigious medical organizations in world, American College of Cardiology and American Heart Association. This program is designed for assisting physicians and patients to assess the risk of atherosclerotic cardiovascular events. Based on the results of risk assessment, advices of medical treatment are provided to reduce the risks. Unlike other clinical tools designed by the organizations primarily for physicians, this tool can also be used by patients themselves.
The advices from this program are very helpful to address some most common issues in the primary prevention of atherosclerotic cardiovascular diseases.
Aspirin Therapy. We have seen the never-ended debates in WeChat community on the daily Aspirin in primary prevention of ASCVD. The risk of gastric and other internal hemorrhage caused by long term use of Aspirin in clinical reports have been heavily quoted. On another hand, its benefit of preventing cardiovascular events is undeniable. As now, no guideline recommends routine aspirin use for primary prevention of CV events. The strategy of shared decision-making to individualize decisions based on CV risk verses bleeding risk is used by USPSTF( US Preventive Services Task Force), ACC/AHA (American College of Cardiology and American Heart Association), Heart Stroke Foundation, European Society of Cardiology, American Diabetes Association and Diabetes Canada (Link). “Shared decision-making? How could I do that?!” you ask. Thus, many people are left wondering if they should be on aspirin, or not. ASCVD Risk Estimator Plus is able to provide the individualized advice of Aspirin Therapy for primary prevention by assessing each patient’s CV risk as well as bleeding risk. As a reminder, ACC and AHA is the parents of ASCVD Risk Estimator Plus.
Statin Therapy. The dosage of statin therapy is not just simply decided by LDL levels. All risk factors, like diabetes, smoke or age, have to be considered. This program provides individual advices for a patient if she or he needs starting a statin medication, and recommends drug intensity, so patients will know their needed dosage according their estimated CV risk levels.
Anti-Hypertension therapy. As mention earlier, the challenge of initiation of a medication for patients with elevating blood pressure in borderline is well known. People would often ask questions: To lower my blood pressure, perhaps, I just need to change my life styles, like exercises, healthy diet, etc., instead of taking medicines. Or, there are so many types of medicines for high blood pressure, which type would be better for me? This program provides advices for those, and more questions.
Some key notes for ASCVD Risk Estimator Plus are:
- It is the assessment of risk and assistance of clinical decision-making for primary prevention. It is not designed for secondary prevention. The risk estimation is not very helpful for people who are under intensive statin or anti-hypertension therapy.
- It is for people at age between 20 and 79.
- Lifetime risk assessment is particularly useful for describing and communicating ASCVD risk in younger individuals (<50 years of age), in whom 10-year risk may be low even when significant risk factors are present, according to the physician-designers of this program.
- The optimal uses of the program in the front page are very helpful for clinicians.
This program consists of three titled pages of Estimate, Advice, and Therapy Impact. It takes less than one minute from keying information to obtaining results.
- Estimate page. It requires keying in the information of: Gender, Race, Age, the values of Total Cholesterol, HDL Cholesterol, LDL Cholesterol: the blood pressure values of Systolic and Diastolic: Yes or No being Diabetic: Yes or No being a Smoker; Yes or No on Anti-Hypertension therapy; Yes or No on Aspirin therapy; Yes or No on Statin therapy
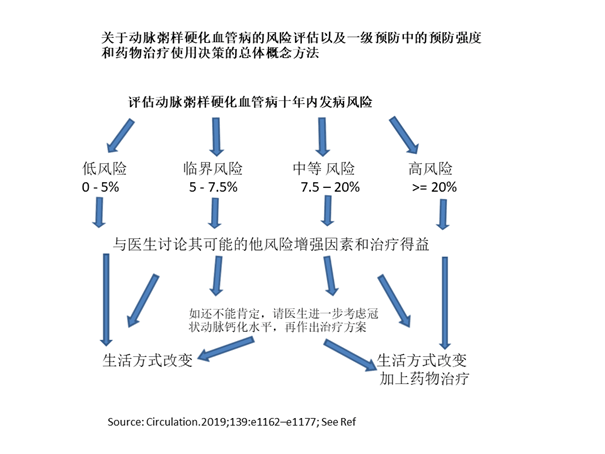
- Advice page. After information keyed in at Estimate page, the Advice page displays the 10-year risk for atherosclerotic cardiovascular disease, which is, within the next 10 years, the probability of the first occurrence of heart attack or stroke. This page also gives suggestions which treatment is needed to reduce the risk. The ASCVD risk is expressed as percentage. <5% is low risk; 5-7% is borderline risk; 7.5-20% is intermediate risk, and ≥20% is high risk.
- Therapy Impact page, it displays how much of risk could be reduced after initiation of the suggested therapy.
Note: Due to the consideration of bleeding risk for Aspirin Therapy, this option for Aspirin Therapy will be switched off if the patient is prone to the bleeding risk.
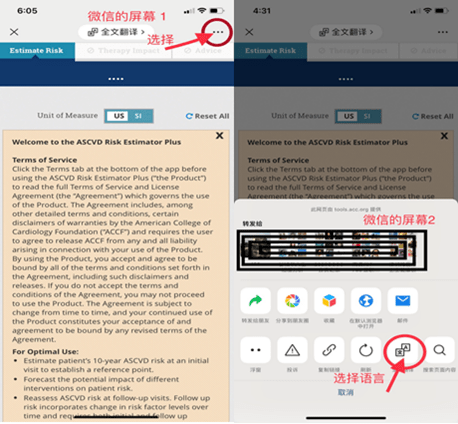
How to change the language for English to Chinese to proceed with ASCVD Risk Estimator Plus
There is App of ASCVD Estimator Plus available to download. Neither App nor website based program are available in Chinese. However, for physicians or patients who prefer the language in Chinese, we are able to utilize the translating function of smart phones as well as that in WeChat, to proceed with the risk assessment directly through the website of American College of Cardiology. The illustrations of how to change the language from English to Chinese are shown as below:
- WeChat users When the originally chosen language for a smart phone is Chinese, please browse through the link https://tools.acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate/, the ASCVD Risk Estimator Plus will appear in English. To change it into Chinese:
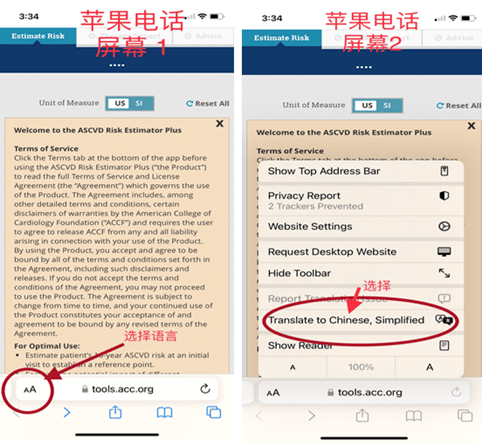
I-Phone users These phones have the applicability of switching the reading from English to Chinese:
Because it is a streamline translation, two technical terms, [Race], [US IS] are not properly expressed. Those translation errors have no negative impact on utilizing the program. Rectification of these errors will be discussed later in illustrations.
ASCVD risk Estimator Plus is not only for patients’ first assessment of their risks, but also for their following assessments. For example, a patient had ASCVD risk score of 25% one year ago, and she took the advices of preventive treatment. She is able to re-assess her current risk after one-year treatment. She may see her risk of heart attack from 25% down to 10%! Then she just could not help to smiling. She needs to provide the program with her previous input information.
As soon as we have landed on the website and changed the language into Chinese, we may start exploring the utilization of this program. https://tools.acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate/
A case of a hypothetical patient is demonstrated below for the purpose of learning. At this point, I believe, you, as a reader of this article, must be an intelligent, educated person. More importantly, you care about the health of your patients, your family members or yours. So I suggest you to use the given information of the hypothetical patient to practice briefly before viewing the illustrating screens. By doing this you will gain the sense of how simple and easy the process is.
Illustration of Case 1
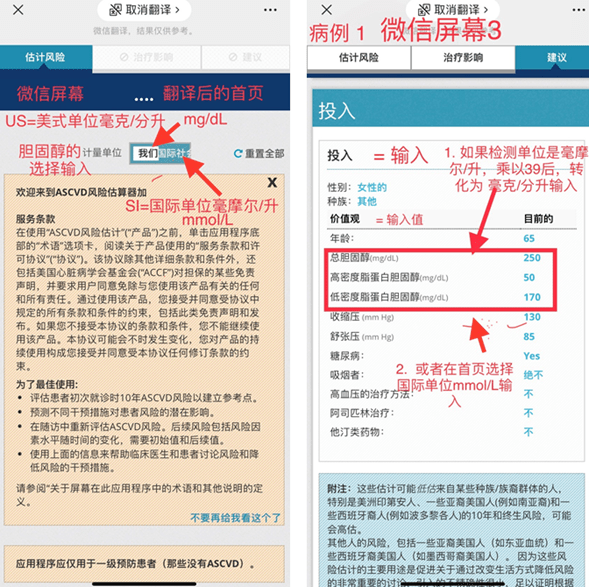
After the language is changed into Chinese, we need to select the Unit of Measure for inputting cholesterol levels. In WeChat screen, the Unit of Measure (计算单位) has two options. On the left it shows 【我们】for the original 【US】, which stands for American System。 It is selected for inputting cholesterol in mg/dL. On the right next to it, it shows 【国际社会】for the original 【IS】, which stands for International System. It is for inputting cholesterol in mmol/L. You makea selection depending on which Unit of Measure is used in your lab result. In I-phone, the first screen in Chinese shows the 计算单位 with a slightly different appearance. On the left,【USSI】is for inputting cholesterol in mg/dL. Next to its right, it is a solid block in blue color, and is for inputting cholesterol in mmol/L. By making one of selections on the first screen, you don’t need to make the math conversion yourself. If needed, the method of conversion is showed in Screen No. 3.
The information for input in the case is:
Age 65; Gender Female; Race Others; Total Cholesterol 250 mg/dL; HDL Cholesterol 50 mg/dL; LDL Cholesterol 170 mg/dL; Blood pressure Systolic 130 mm Hg and Diastolic 85 mm Hg; History of Diabetes Yes; Smoker No; Hypertension Treatment No; On Aspirin Therapy No; On a statin No
Note:Input【竞赛】 = 人种
The program also asks if it is a following up for re-assessment of risk after treatment. For an initial assessment, select “No”. If it is a re-assessment, select “Yes” and the previous data are needed.
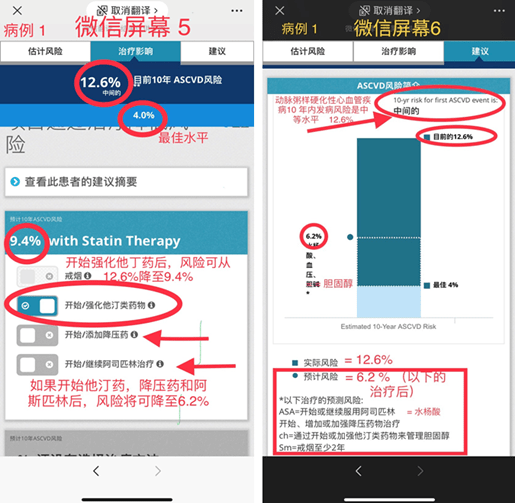
After have the required information inputted, press 【建议】key (Advice key). The estimated 10 year-risk of first occurrence of atherosclerotic cardiovascular event in probability is displayed. This lady has the risk of 12%. A healthy individual has an optimal risk of 4%. (Please note: if this lady is not diabetic, with her current cholesterol level and blood pressure level, she would have the risk of 6.7%). The program suggests this lady need treatments of lowering her LDL cholesterol and her high blood pressure and taking low dose aspirin. For treatment of diabetes, this program is not able to provide advices and the lady needs to consult her endocrinologist. Information for health life style and safety of treatment are provided. Press 【全部展开】,the program provides details of preferred treatments and the source of particular items from treatment guideline.
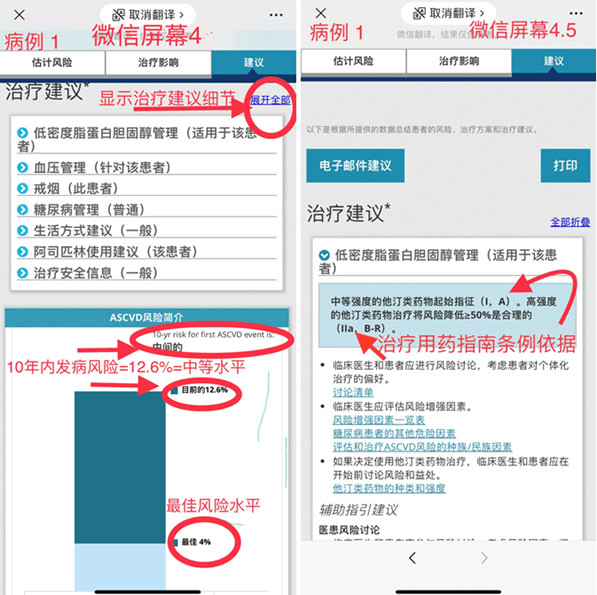
Press 【治疗影响】(Therapy Impact) and select 【启动/强化他汀类药物】,the risk could be reduced from 12.6% to 9.4%. Select 【启动/强化抗高血压药物】, the risk could be reduced from 12,6% to 9.2%. Select both, the risk could be reduced to 6.9%. If the lady starts all three suggested treatments, statin therapy and hypertension treatment as well as aspirin therapy, the risk could be reduced further lower to 6.2%.
The advice from ASCVD Estimator Plus is greatly valuable for clinicians and patients to estimate the benefits of preventive drug treatments. But it is not a replacement of clinicians’ professional judgement. Clinicians are able to evaluate other interconnected factors, such as “Risk-Enhancing Factors”. The Risk-Enhancing Factors include Family history, Kidney disease, hypertriglyceridemia, chronic inflammatory conditions, etc…. They are not taken into account in the risk-assessment of this program. If having those Risk-Enhancing Factors, people would have the actual risk of heart attack or stroke higher than the estimated risk predicted by this program. In addition, clinicians are able to individualize treatments according patients’ conditions. The designing physicians of this program gave an example in case that a broader consideration is needed. Some patients have very high blood pressure as well as high cholesterol and taking aspirin. Those patients have higher risk of hemorrhage stroke. Physicians may be better to focus on lowering blood pressure to prevent hemorrhagic stroke. Statin therapy can be started later. The decisions of a treatment adjustment like this can only be made by clinicians.
The Final Comment
At present, thankfully we have a tool to predict the probability of heart attack or stroke within 10 years or life time risk. It has always been difficult to convince ourselves or others to take preventive actions for a health condition. We tend not to seek for help until we suffer. Before struck by stroke, one might be perfectly feeling fine, healthy or even agile. At a dinner party, one would sneer at you as a fool if you try to persuade him away from Mao Tai due to the concern of his high blood pressure. This ASCVD Risk Estimator Plus helps us aware of the multitude of the hidden risks. Hence, it motivates us to take actions, to prevent ourselves from the future devastations.
Reference:
Use of Risk Assessment Tools to Guide Decision-Making in the Primary Prevention of Atherosclerotic Cardiovascular Disease: A Special Report From the American Heart Association and American College of Cardiology Donald M. Lloyd-Jones, Lynne T. Braun, Chiadi E. Ndumele, Sidney C. Smith Jr, Laurence S. Sperling, Salim S. Virani and Roger S. Blumenthal Circulation. 2019;139:e1162–e1177